![]()
What is shoulder bursitis and impingement?
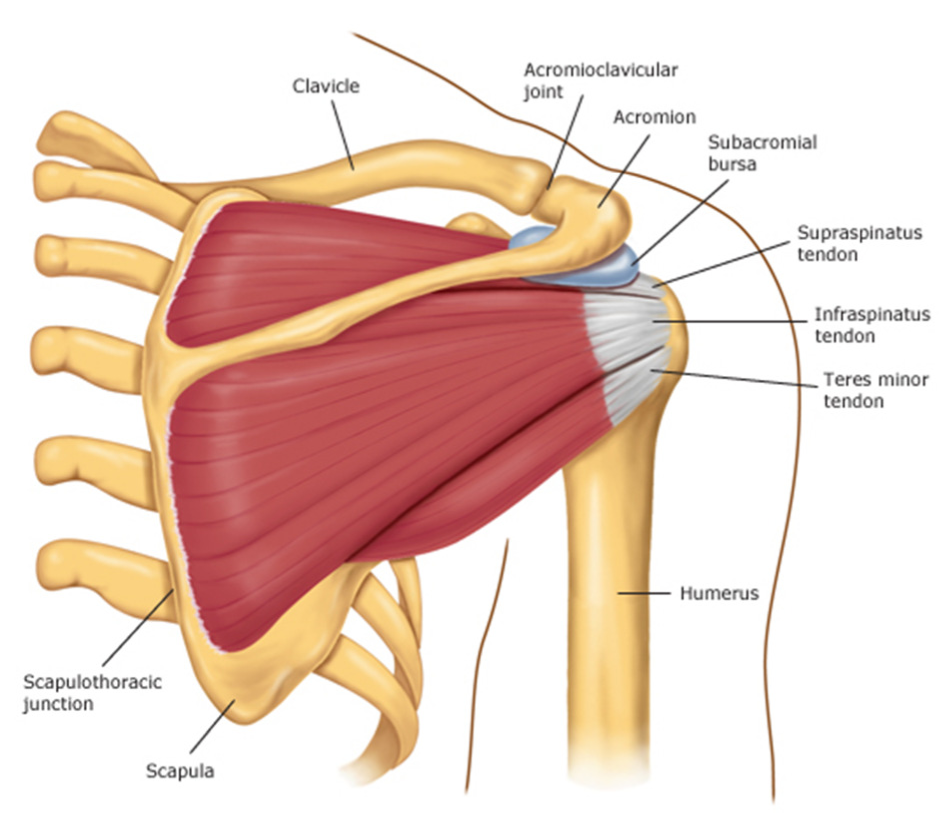
The shoulder joint is comprised of three bones – the humerus (armbone), the scapula (shoulder blade), and the clavicle (collarbone). The ball-and-socket part of the shoulder joint is made up of the ball end of the humerus, and the socket end of the scapula (glenoid). The scapula has a bony protuberance called the acromion which overhangs the humerus. Between the shoulder joint and the acromion is a bursal sac called the subacromial bursa. This bursa contains fluid and helps cushion the shoulder joint and the rotator cuff beneath it.
How is shoulder impingement and bursitis caused?
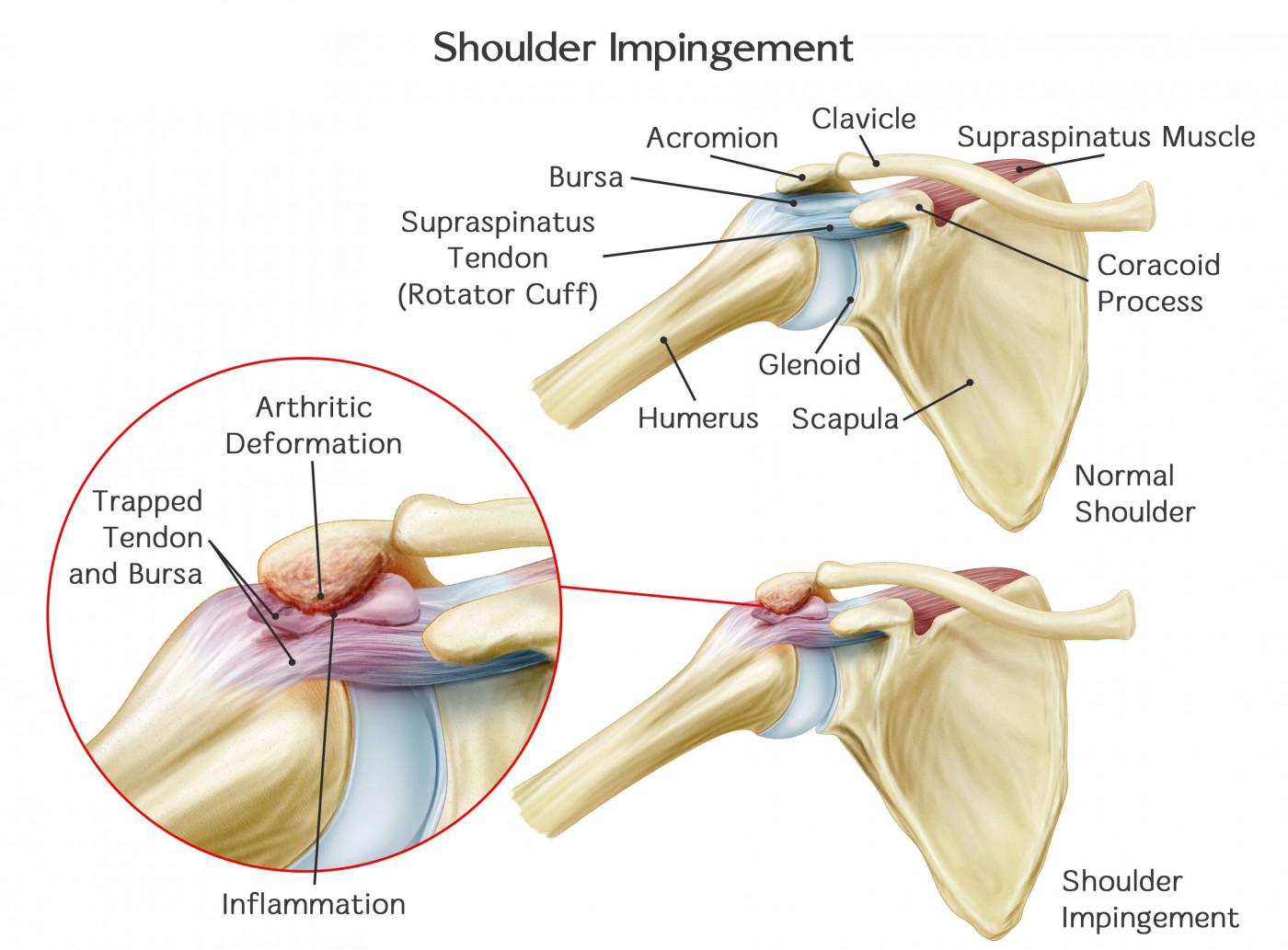
With repetitive strain the subacromial bursa can become thickened, inflamed and painful. In addition, the bony acromion of the shoulder blade can protrude into the bursa due to its curved shape or because of bone spurs. When the arm is brought overhead, the bony humerus and the overlying rotator cuff tendon can become caught or ‘impinged’ on the acromion. This can be thought of as a thick shag rug getting caught under a door. Thickened ligaments and tendons around the shoulder can also contribute to this shoulder impingement.
What are the symptoms of shoulder impingement and bursitis?
Shoulder impingement and subacromial bursitis can cause the following problems:
- Pain in the shoulder which is worse with overhead arm movements.
- Clicking and catching of the shoulder with movement
- Difficulty with overhead tasks
How is shoulder impingement and bursitis diagnosed?
A detailed history and clinical examination is required to assess the range of motion of the arm and strength of the shoulder muscles. Additional tests include:
- X-ray of the shoulder – this enables assessment of the shape of the bony shoulder and presence of bony spurs.
- Ultrasound – a simple test that can help identify an inflamed subacromial bursa.
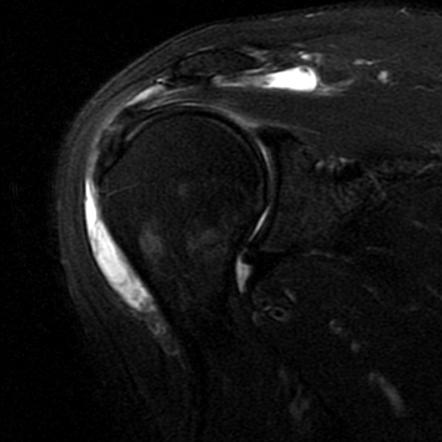
- MRI – the gold standard in imaging to show in detail condition of the soft tissue, including the bursa and rotator cuff tendons.
How is shoulder impingement and bursitis treated?

Subacromial bursitis and shoulder impingement can respond to non-operative management. This includes resting the shoulder from aggravating activities and overuse. Anti-inflammatory medications can also be useful for pain relief. Physiotherapy can also be beneficial to maintain flexibility and range of motion in the shoulder, and to strengthen the muscles around the shoulder. Occasional ultrasound guided injections of steroid can also be prescribed to aid in pain management.
If these non-operative measures do not improve the symptoms and the pain continues to limit daily activities, then surgery may be an option. Click below to read more about subacromial decompression and acromioplasty for impingement.Click here
My goals as a surgeon are to relieve your pain, restore your function, and return you back to doing what you love.
– Dr Raymond Yu
- Adelaide Orthopaedic Surgeon
- Adelaide Shoulder Surgeon
About
Dr Raymond Yu
Dr Raymond Yu is an Adelaide Orthopaedic Surgeon with post-Fellowship expertise in Shoulder and Elbow Surgery.
He specialises in orthopaedic surgery of the Shoulder and Upper Limb with a focus on modern keyhole and minimally-invasive techniques.
Dr Yu has a special passion for:
- Rotator cuff repair surgery
- Shoulder replacement surgery
- Shoulder stabilisation surgery
Dr Yu practices at



